
The pH Problem at the Heart of Eczema

In atopic dermatitis, a single biochemical disruption — the loss of skin surface acidity — cascades into barrier failure, microbial dysbiosis, and chronic itch. Understanding and correcting it may be the missing piece in long-term disease control.
Author: Dr. Rafal Pielak
Most conversations about eczema begin with inflammation. The redness, the immune cascade, the cytokines — these are the visible, measurable, pharmacologically targetable features of atopic dermatitis (AD), and they have appropriately commanded much of the field’s attention (1,2). But upstream of the inflammation, before the immune system fully mobilizes, something more fundamental goes wrong: the skin surface becomes less acidic than it should be (3,4).
This shift is not merely a consequence of the disease—it is a key driver of it. Elevated skin surface pH disrupts the enzymes responsible for barrier formation, activates proteases that degrade it, shifts the microbial balance toward pathogenic species, and triggers molecular pathways that sustain chronic itch (5–10). It represents a biochemical fault line that cuts across nearly every pathogenic axis of atopic dermatitis (11,12).
Understanding why skin pH rises in AD, what it sets in motion, and how restoring physiological acidity can interrupt these cascades offers a coherent, mechanistically grounded framework for a disease that remains difficult to control long-term.
A Number That Should Not Rise
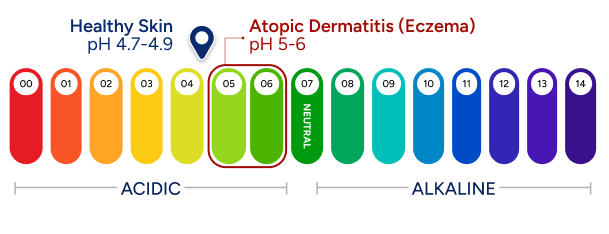
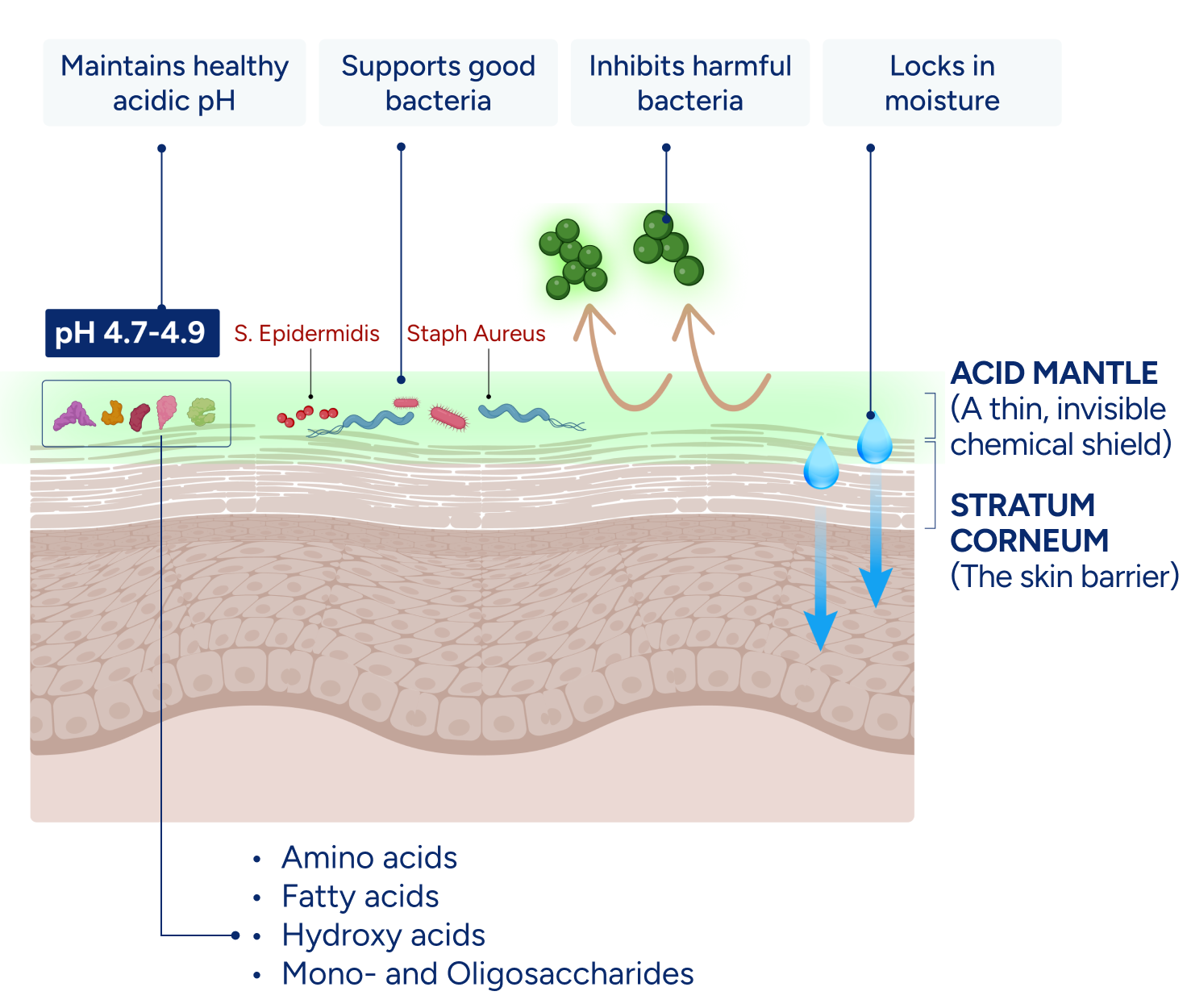
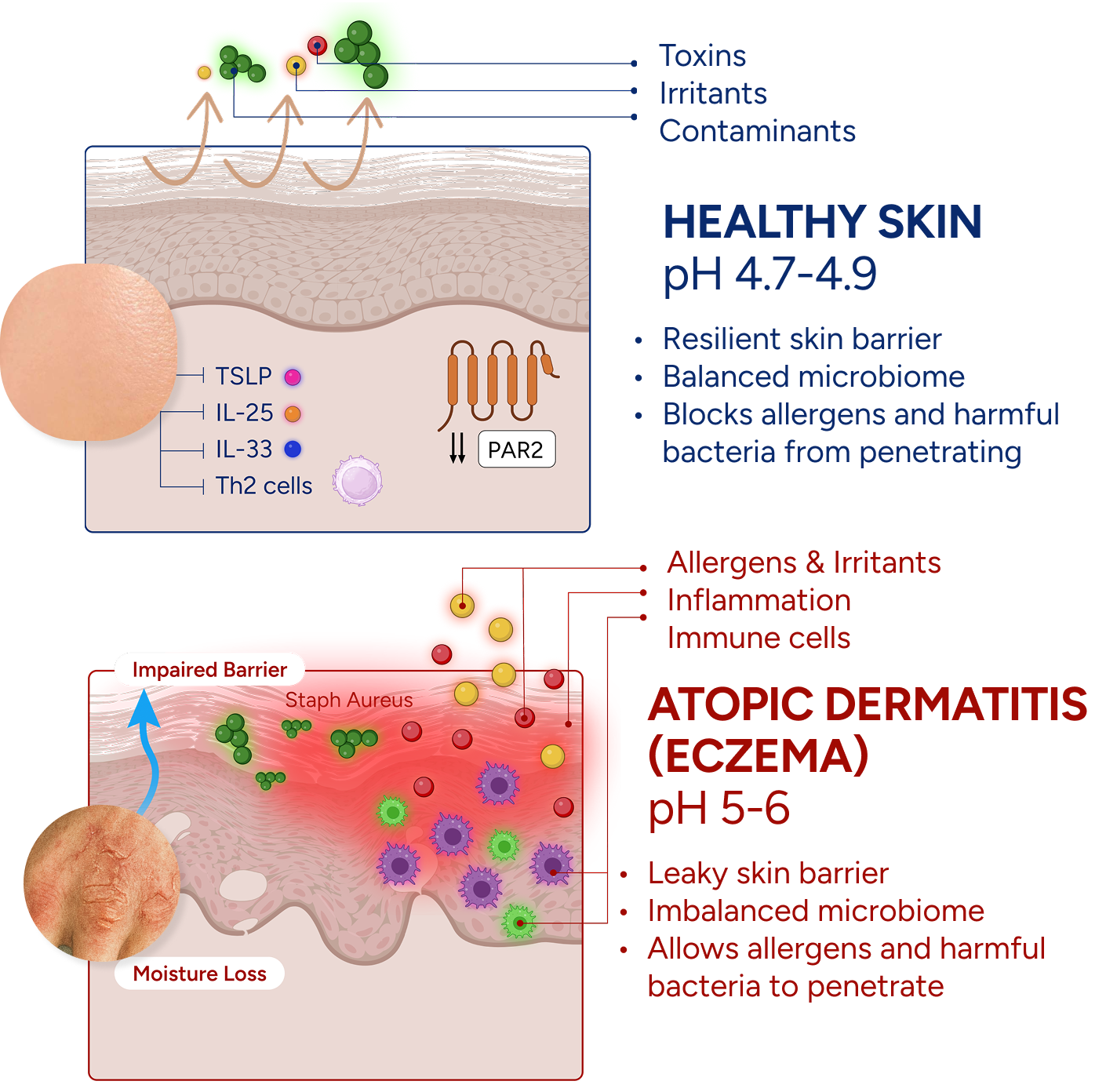
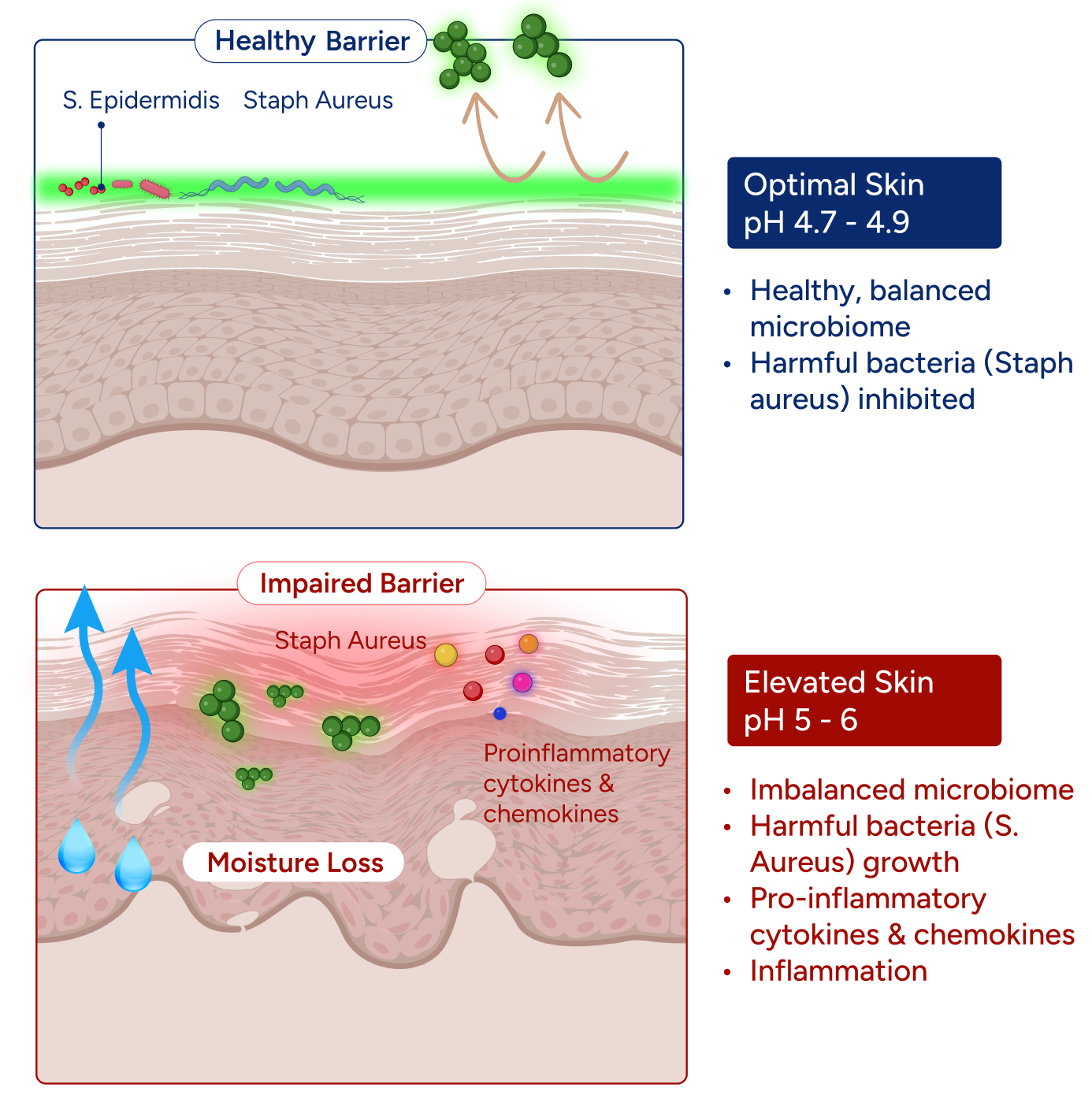
Healthy human skin maintains its surface within an acidic range, with an optimal pH of approximately 4.7 (3). This is not incidental — it is biochemically necessary. The enzymes responsible for building the skin's lipid barrier, the inhibitory systems that keep barrier-degrading proteases in check, and the ecological conditions that favor beneficial microbes over pathogens all depend on that narrow acidic window (5,6,11). The acid mantle — a thin, dynamic film of free fatty acids, amino acid derivatives, lactic acid, and microbial metabolites — sustains this environment continuously, buffering against alkalinizing perturbations from water, cleansers, and environmental exposure (3,12).
In atopic dermatitis, this system is chronically compromised. Skin surface pH is frequently elevated, and this elevation is not merely a consequence of disease—it is an upstream driver. It impairs barrier formation, activates destructive proteases, and reshapes the microbial community before visible inflammation emerges (5,8,13).
“Elevated skin surface pH is not a side effect of atopic dermatitis.
It is an upstream driver — one that impairs the barrier, activates destructive proteases, and shapes the microbial community before visible inflammation appears.”
Filaggrin: The Protein That Holds the Acid Mantle Together
The most significant molecular contributor to pH dysregulation in atopic dermatitis is filaggrin deficiency (4,14). Filaggrin is a key structural protein of the epidermis that undergoes controlled proteolytic breakdown during terminal keratinocyte differentiation, generating the components of natural moisturizing factor (NMF)—including free amino acids, pyrrolidone carboxylic acid (PCA), urocanic acid, and other polycarboxylic molecules (15,16). These NMF constituents serve two essential functions: they attract and retain water within the stratum corneum, and they help acidify and buffer the skin surface (12,15). Together, they represent a central input into the acid mantle.
When filaggrin is reduced or absent—whether due to loss-of-function mutations in the FLG gene or suppression of its expression by Th2 cytokines such as interleukin-4 (IL-4) and interleukin-13 (IL-13)—both NMF levels and surface acidification decline in parallel (14,17–19).
Importantly, IL-4 and IL-13 suppress filaggrin expression even in individuals without FLG mutations (17,19). This means that the inflammatory state of atopic dermatitis can drive and sustain pH dysregulation independently of genetic predisposition. In this context, elevated skin pH is not only a downstream consequence but also a biochemical extension of the Th2 immune response itself. The result is a self-reinforcing loop in which inflammation raises skin pH, and elevated pH, in turn, amplifies inflammation (5,7).
pH Dysregulation Across the Arc of Disease
pH disruption in atopic dermatitis is not a single event—it plays distinct roles in both the initiation of disease and its long-term persistence.
Disease Initiation: When the Acid Mantle Fails First
In early atopic dermatitis, often presenting in infancy or early childhood, a convergence of factors—filaggrin deficiency, immature barrier architecture, and environmental alkalinizing exposures (such as soaps, hard water, and surfactants)—creates conditions in which the acid mantle cannot be adequately maintained (4,14,20). Even before overt inflammation develops, pH-dependent barrier processes begin to fail: ceramide synthesis slows, kallikrein activity increases, and the skin becomes structurally vulnerable (5,6).
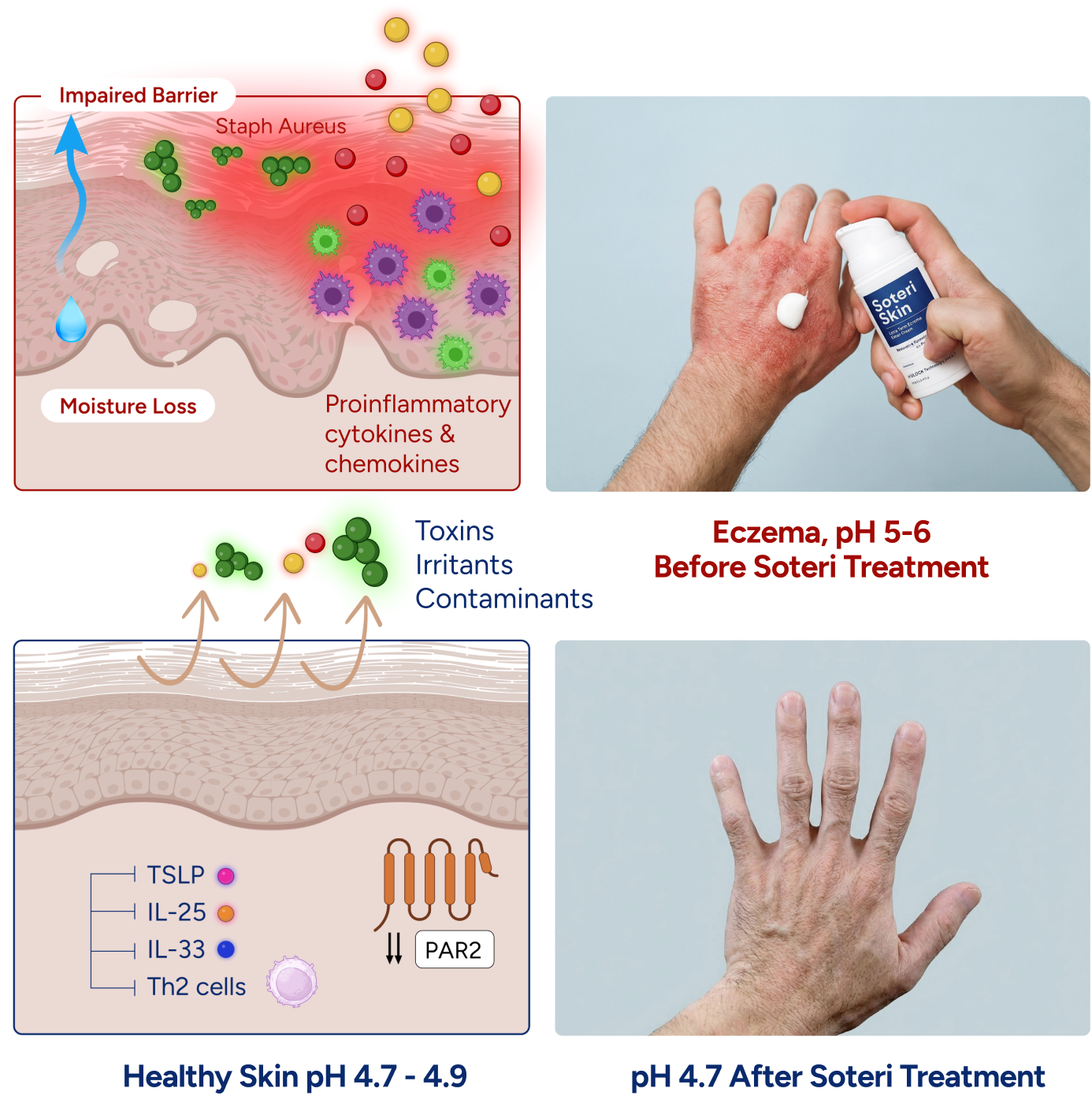
This early barrier disruption creates the conditions for immune priming. Allergens penetrating a compromised stratum corneum encounter dendritic cells and mast cells in the viable epidermis. Keratinocytes under mechanical and chemical stress release thymic stromal lymphopoietin (TSLP), interleukin-33 (IL-33), and interleukin-25 (IL-25)—epithelial “alarmins” that activate innate lymphoid cells and polarize the adaptive immune response toward a type 2 profile (21–23).
At this stage, elevated pH acts as a permissive upstream factor. It does not directly trigger the immune response but removes the biochemical safeguards that normally preserve barrier integrity and limit allergen penetration (7,12).
The atopic march—the progression from early eczema to aeroallergen sensitization, asthma, and allergic rhinitis—has been linked to transcutaneous allergen sensitization through a compromised skin barrier (24,25). Experimental models show that alkalinization of the stratum corneum accelerates this process, while acidification inhibits it (26,27). In this context, the acid mantle functions as a critical gatekeeper of systemic allergic disease.
Chronic Disease : The Self-Sustaining Alkaline State
In established chronic atopic dermatitis, pH dysregulation is no longer just a vulnerability—it becomes a driver of disease persistence. The inflammatory state itself, through IL-4 and IL-13–mediated suppression of filaggrin and other barrier proteins, reduces the skin’s intrinsic ability to maintain an acidic surface (7,17,19). In effect, inflammation suppresses the very mechanisms required to restore normal pH.
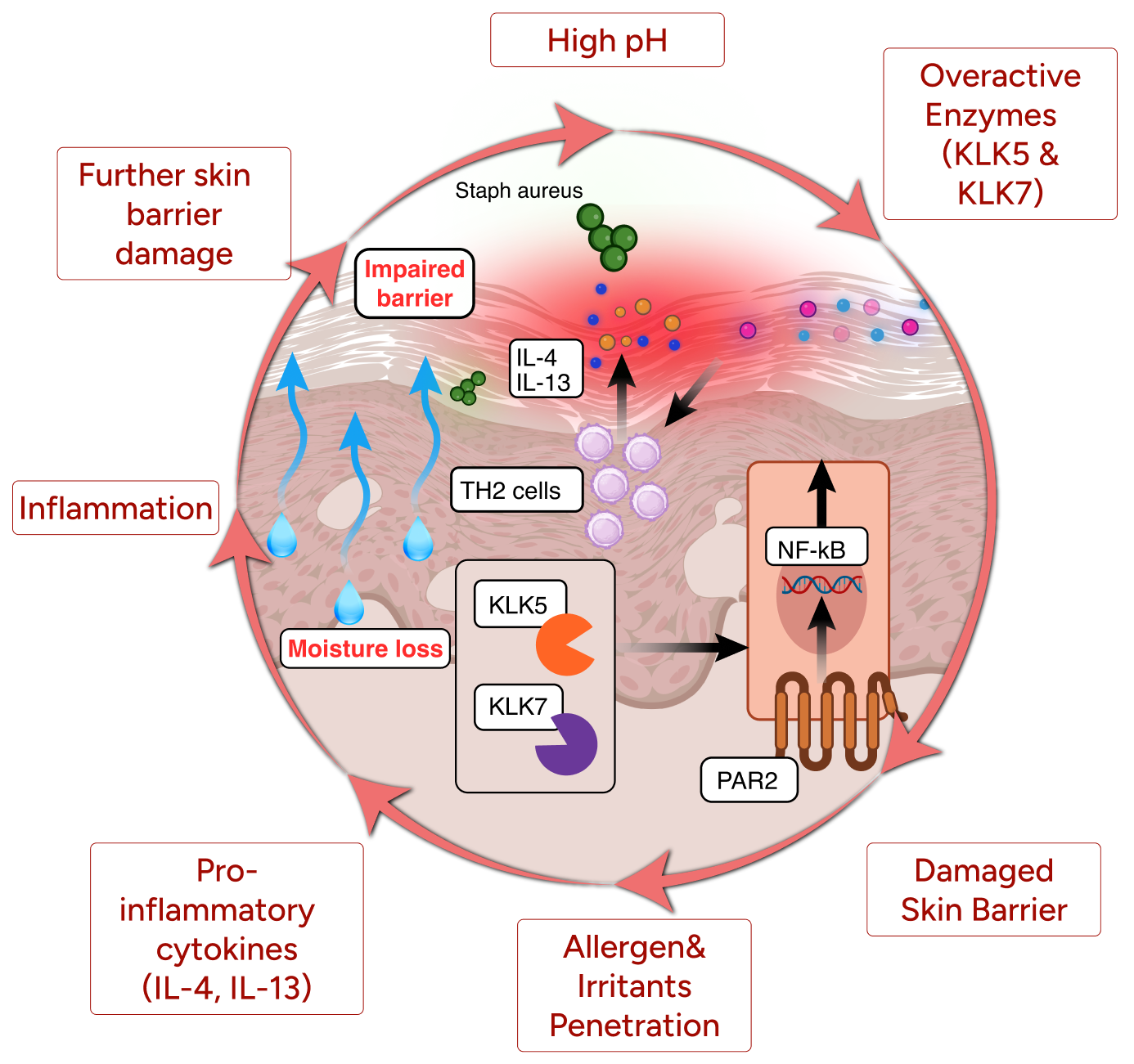
This creates a self-reinforcing cycle: inflammation sustains an elevated pH, and elevated pH further amplifies inflammation (5,27).
Chronically elevated pH maintains activation of the KLK5/KLK7–PAR2 signaling axis, linking barrier degradation to persistent neuronal sensitization (9,13). Over time, neuropeptides such as substance P and calcitonin gene-related peptide (CGRP), together with cytokines like IL-31, lower the activation threshold of sensory neurons and promote spontaneous itch signaling—progressively independent of acute inflammatory triggers (10,28,29).
Itch then becomes self-perpetuating: scratching damages the barrier, further elevates pH, activates proteases, enhances PAR2 signaling, and deepens neuronal sensitization (10,30). The alkaline microenvironment is the biochemical substrate that enables this cycle to persist.
Correcting the pH: What Works and What Doesn’t
A growing body of evidence demonstrates that restoring an acidic skin surface can provide therapeutic benefit in atopic dermatitis (6,12,26). Both preclinical and clinical studies have shown that lowering skin pH can improve barrier function, reduce transepidermal water loss (TEWL), suppress serine protease activity, and limit colonization by pathogenic bacteria such as S. aureus (3,5,31). In murine models, acidification of the stratum corneum accelerates barrier recovery and reduces inflammation, while alkalinization has the opposite effect (26,32). Early clinical studies in humans have similarly reported improvements in barrier integrity and disease severity with acidifying interventions (33,34). Together, these findings support the concept that pH correction is not merely cosmetic—it is mechanistically therapeutic.
However, not all approaches to acidification are equivalent. Dilute vinegar soaks and acetic acid solutions have been explored clinically, and their limitations are instructive (35,36). Controlled studies of dilute vinegar have shown no sustained improvements in barrier function, TEWL, microbial composition, or clinical outcomes in AD, despite achieving measurable short-term reductions in surface pH (35). In these studies, skin pH returned to baseline within approximately 60 minutes of application.
The limitation is not that acidification is ineffective—it is that transient acidification is not the same as restoring the acid mantle. Atopic skin does not simply require a temporary drop in pH; it requires a stable buffering system centered around the physiological range (~pH 4.7) that can resist alkaline drift over hours, not minutes (3,12).
Effective therapeutic acidification therefore depends on formulation design. It requires buffering systems composed of weak acids with pKa values near the target pH, combined with molecular properties that limit rapid penetration into the stratum corneum. This ensures that the acidifying components remain at the skin surface, where they can continuously buffer against external and endogenous alkalinizing forces (6,34).
In this context, the goal is not to transiently lower the skin pH, but to re-establish a durable, self-stabilizing acidic environment—one that restores the biochemical conditions necessary for barrier integrity, microbial balance, and immune regulation.
“Transient acidification is not the same as acid mantle restoration. What atopic skin needs is sustained buffering capacity centered near pH 4.7 — a system that resists alkaline drift over hours, not minutes.”
Soteri Skin: From Transient Acidification to Sustained pH Correction
Most moisturizers are designed to provide temporary soothing relief, but they do not actively restore the skin barrier. Moreover, many are formulated at a pH that is too high for atopic skin, which may further impair barrier function and disrupt skin health. Even products labeled as “pH-balanced” are typically formulated around pH ~5.5, which may be appropriate for general skincare but remains too alkaline for atopic dermatitis, where the optimal functional range is closer to pH 4.7.At this higher pH, key barrier enzymes remain suboptimal, serine proteases are insufficiently suppressed, and the microbial environment continues to favor pathogenic species.
In other words, many moisturizers hydrate the skin—but do not correct the underlying biochemical conditions that drive disease.
Soteri Skin was developed to address this gap. At the core of the formulation is the pH/LOCK® complex, a buffering system specifically engineered to not only lower skin surface pH to the optimal ~4.7, but to maintain it within this range for 12+ hours. This is a critical distinction. Rather than providing a transient drop in pH, the pH/LOCK® system establishes a stable, surface-resident buffer that resists alkaline drift from environmental exposures, washing, and endogenous processes.
By maintaining the skin within this optimal acidic window, the formulation restores the biochemical conditions required for:
Efficient lipid processing and barrier repair
Suppression of kallikrein protease activity
Support of a healthy microbial ecosystem
Reduction of inflammatory signaling and itch pathways
This mechanistic approach is supported by clinical data. In a prospective clinical study, treatment with Soteri Skin resulted in a 92% reduction in disease severity, as measured by the Eczema Area and Severity Index (EASI). Notably, 70% of patients achieved near-complete symptom relief, and participants reported an 82% improvement in quality of life over six weeks of treatment (37).
These results highlight an important principle: when skin pH is corrected and stabilized, multiple downstream pathogenic pathways improve simultaneously, restoring the skin’s native regulatory environment and re-establishing control over the processes that drive atopic dermatitis.
“Soteri Skin restores and stabilizes skin pH, reactivating the skin’s intrinsic ability to repair, regulate, and protect itself across all major pathways of atopic dermatitis.”
Acid Mantle Restoration as a Combination Therapy
Current immunomodulatory therapies for atopic dermatitis—topical corticosteroids, calcineurin inhibitors, PDE4 inhibitors, JAK inhibitors, and biologics targeting type 2 cytokines—are highly effective at suppressing immune signaling and inflammation. However, these therapies do not directly correct the underlying biophysical abnormalities of atopic skin: elevated pH, impaired ceramide synthesis, excessive protease activity, and microbial imbalance. As a result, many patients—even those treated with biologics—continue to experience residual xerosis, subclinical barrier dysfunction, and susceptibility to flares. Persistent pH elevation in these patients may sustain protease activity and microbial dysbiosis even as inflammatory cytokine levels decline.
This is where sustained pH correction becomes complementary. By restoring skin surface pH to its optimal range, the biochemical conditions required for barrier repair are re-established. In patients using topical corticosteroids or calcineurin inhibitors, normalized pH enhances the barrier-rebuilding processes that anti-inflammatory therapies make possible. Ceramide synthesis becomes more efficient, and protease-driven degradation of corneodesmosomes is reduced. The result is an environment in which true barrier repair can occur—potentially allowing for earlier tapering of anti-inflammatory treatments while maintaining clinical stability.
In patients treated with JAK inhibitors, which block intracellular signaling pathways involved in inflammation and itch, sustained pH normalization adds an orthogonal mechanism of action. It suppresses extracellular protease activity and PAR2-mediated sensory signaling—pathways that may persist despite cytokine inhibition. Similarly, in patients receiving biologics, acid mantle restoration addresses residual biochemical dysfunction not corrected by cytokine blockade alone, supporting lipid maturation, promoting a commensal-dominant microbiome, and reducing itch signaling independently of IL-4/IL-13 activity.
“Immune-targeted therapies suppress inflammation. Sustained pH correction repairs the substrate in which inflammation operates — the barrier, the microbiome, the sensory environment. Together, they address dimensions of the disease that neither reaches alone.”
Importantly, the safety profile of pH-modulating approaches supports their use across all stages of disease and across age groups. As non-immunosuppressive interventions, they are well tolerated and suitable for continuous use—during both active treatment and remission. This positions acid mantle restoration as a foundational component of care: not a replacement for pharmacologic therapy, but a complementary strategy that enhances its effectiveness and supports more durable disease control.
Conclusion: Restoring the Missing Axis
Atopic dermatitis is often treated as an immune disorder, but at its core it is also a disorder of lost biochemical regulation at the skin surface. Elevated pH sits upstream of barrier failure, microbial imbalance, and chronic itch—linking these processes into a single, self-reinforcing system. Correcting and stabilizing skin pH offers a unifying intervention: one that restores the conditions under which the skin can repair, defend, and regulate itself. In this light, acid mantle restoration is not an adjunct—it is a foundational strategy for achieving durable control of eczema.
References