
The Skin Layer You’ve Never Heard Of Is Controlling Your Barrier

A thin, invisible film on your skin surface controls how your barrier is built, which microbes thrive, and why eczema keeps coming back. Meet the acid mantle.
Author: Dr. Rafal Pielak
There is a layer on your skin you will never see, never feel, and almost certainly have never thought about. It has no official organ status. It does not appear in anatomy textbooks. Yet it quietly governs some of the most important biochemistry happening at your body’s surface, every second of every day.
It is called the acid mantle.
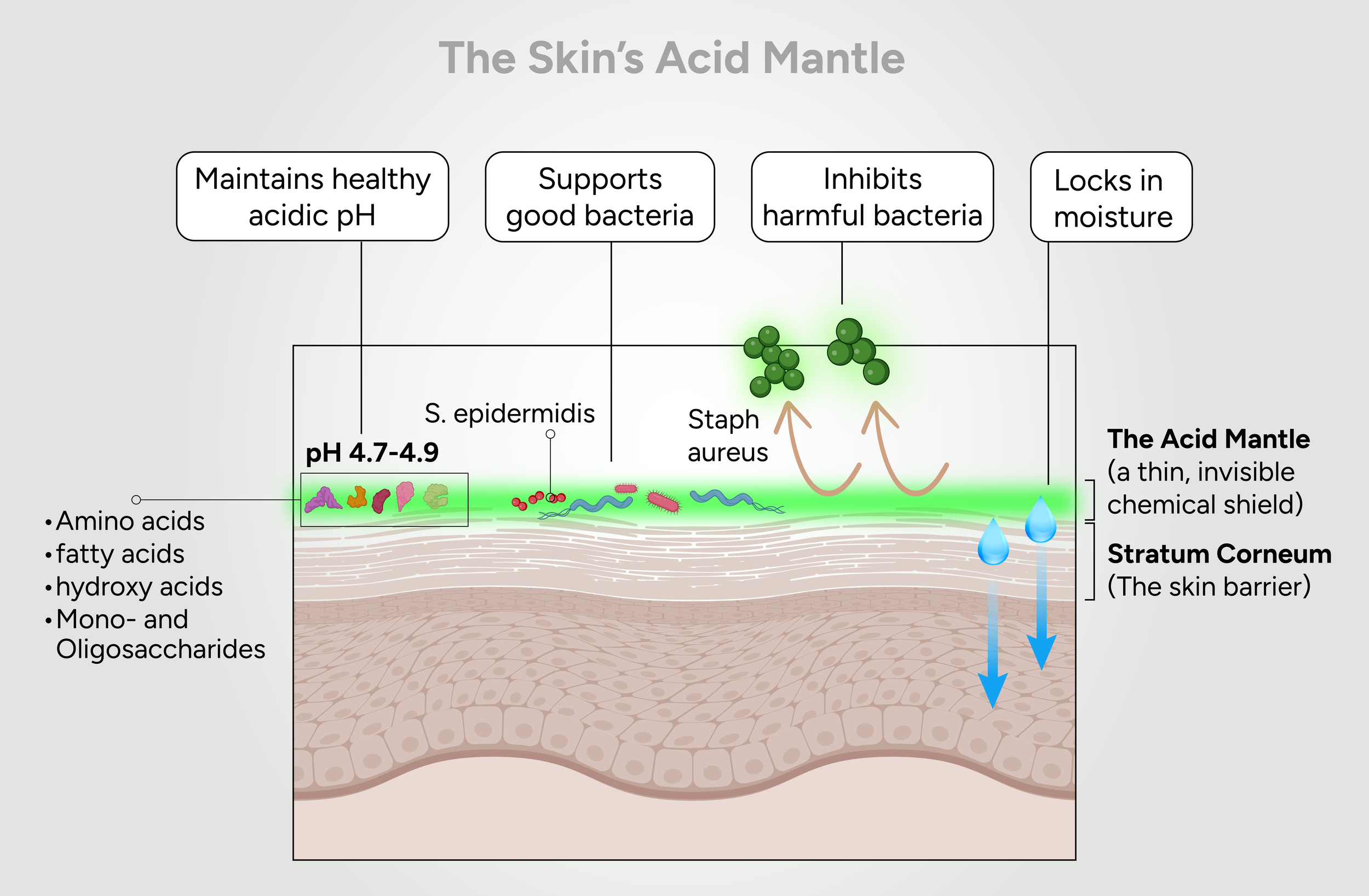
The acid mantle is a biochemical film that coats the outermost layer of the skin — the stratum corneum. It is not a single substance but a dynamic mixture: free fatty acids from sebum and lipid metabolism; amino acids and hydroxy acids, including pyrrolidone carboxylic acid and trans-urocanic acid, derived from the breakdown of the structural skin protein filaggrin; lactic acid from sweat glands; and short-chain fatty acids produced by the microbes living on your skin. Together, these components establish and maintain the skin’s naturally acidic environment. Importantly, they do more than simply determine pH — collectively, they function as a buffering system that actively resists shifts in pH and helps preserve the biochemical stability of the skin surface (Fluhr and Elias 2002, Pielak and Maibach 2022, Tan and Lio 2025).
“The acid mantle does not merely sit on top of the barrier. It creates the conditions under which the barrier can be built.”
Why pH Matters More Than You Think
pH regulation is central to life. Enzymatic active sites frequently contain amino acid residues whose protonation state determines catalytic activity. Even slight deviations in pH can alter enzyme conformation, substrate binding, and reaction kinetics. For this reason, organisms expend substantial metabolic energy to maintain compartment-specific pH homeostasis.
Human blood, for example, is tightly regulated between pH 7.35 and 7.45. Deviations outside this narrow window can rapidly become life-threatening, with cascading effects on oxygen binding, cardiac excitability, and metabolic enzyme function. At the cellular level, the compartmentalization of pH is even more striking: the cytoplasm is maintained near pH 7.2, optimized for glycolytic and biosynthetic enzymes; lysosomes sit at pH 4.5–5.0, enabling the acid hydrolases that break down macromolecules; the mitochondrial matrix is slightly alkaline, the intermembrane space more acidic. Each compartment has a set point. Each set point is defended.
The skin is no different. Its surface pH optimum sits between 4.5 and 5.0 — a range that is not arbitrary but biochemically necessary. What makes the skin unusual is that, unlike a lysosome or the bloodstream, it is an open system. The skin surface is continuously exposed to tap water, surfactant-based cleansers, sweat, friction, UV radiation, pollutants, and microbial colonization. Maintaining a stable pH under these conditions requires a dedicated regulatory architecture. That architecture is the acid mantle (Lambers et al. 2006, Fluhr and Elias 2002, Pielak and Maibach 2022).
The Barrier Is Built From pH Up
The stratum corneum is often described as a brick wall: corneocytes are the bricks, and a matrix of lipids — ceramides, cholesterol, and free fatty acids — is the mortar. This lipid matrix is what makes the barrier waterproof and keeps irritants out. Compromise it, and water evaporates freely from the skin surface while environmental triggers penetrate inward.
Building that lipid matrix requires enzymatic activity. Two key enzymes — β- glucocerebrosidase and acidic sphingomyelinase — process precursor lipids into the ceramides that form the mortar. Both enzymes function optimally under acidic conditions. Elevate the pH and their activity falls. The lipid matrix becomes disorganized. The barrier becomes leaky. Transepidermal water loss increases.
This is not theoretical. Experimental models have demonstrated that acidification improves lamellar lipid assembly, while sustained alkalinization degrades lipid-processing enzymes and compromises barrier integrity. In vitro work has confirmed that acidic pH is required for multilamellar lipid assembly — the very structure that gives the barrier its function (Takagi et al. 1999; Hachem et al. 2003, Hachem et al. 2010).
Proteases, pH, and the Shedding That Shouldn’t Happen
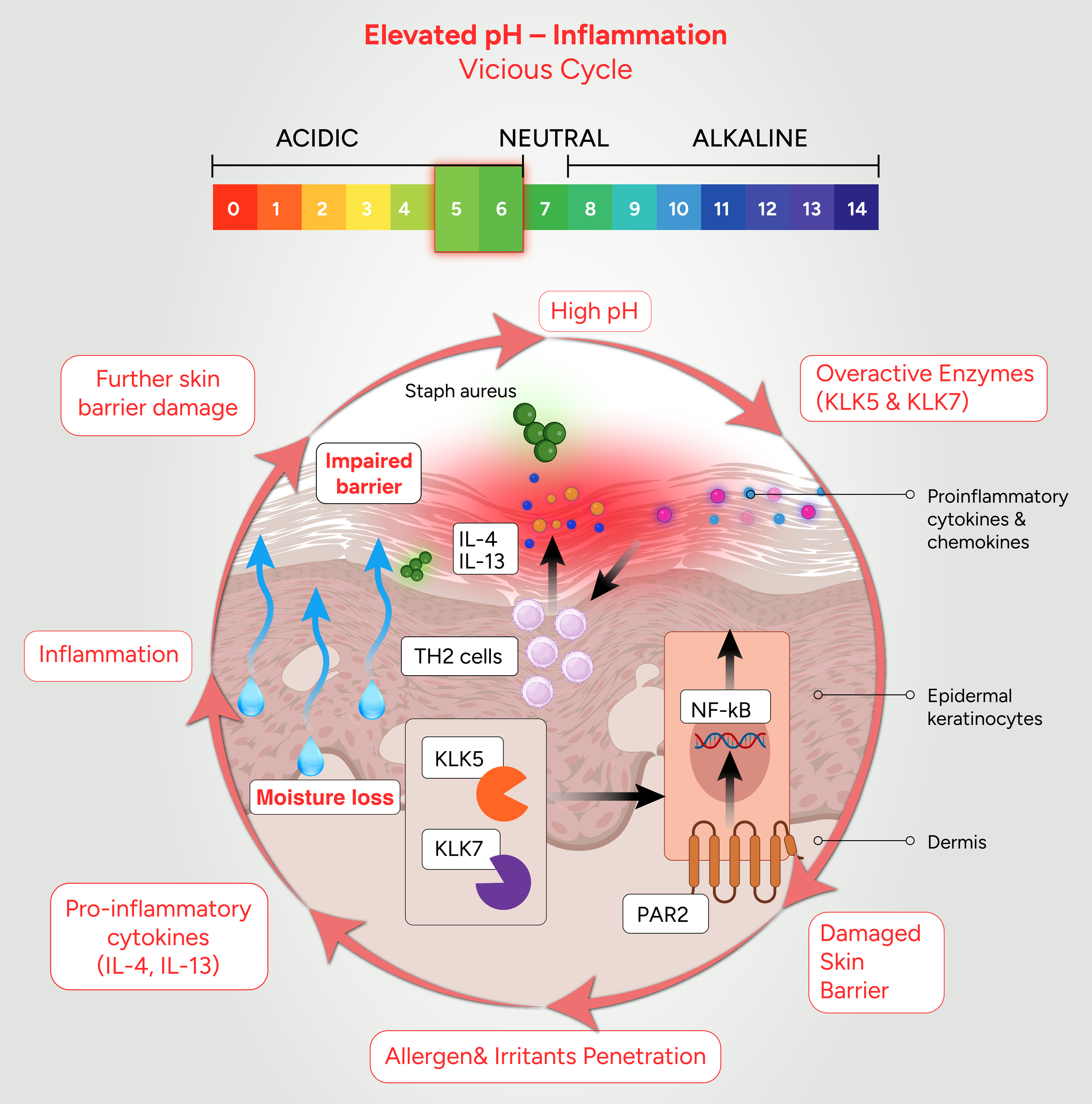
Skin renews itself through desquamation — the orderly shedding of the outermost corneocytes as new cells push up from below. This process is regulated by serine proteases, specifically kallikreins 5 and 7 (KLK5 and KLK7), whose job is to dissolve the protein structures — corneodesmosomes — that hold corneocytes together, releasing them at the right time and in the right sequence (Brattsand et al. 2005, Hachem et al. 2006).
Kallikreins are pH-sensitive. At the normal acidic skin surface, they are kept in check by a natural protease inhibitor called LEKTI, encoded by the SPINK5 gene. LEKTI binds and suppresses kallikrein activity — but only under acidic conditions. As pH rises, LEKTI’s binding affinity weakens, and the proteases are released from inhibition. Corneodesmosomes are cleaved prematurely. The barrier becomes structurally compromised, fragile, and permeable (Hachem et al. 2006)
The consequences extend beyond structural failure. Overactive kallikreins activate protease-activated receptor 2 (PAR2), a receptor expressed on sensory neuronsg and keratinocytes. PAR2 activation triggers the release of thymic stromal lymphopoietin (TSLP) — a key driver of the type 2 immune response that characterizes atopic dermatitis — and directly activates itch-sensing neurons (Briot et al. 2009, Steinhoff et al. 2003).
“Elevated skin pH drives kallikrein overactivity, which activates PAR2, which triggers both itch and immune activation. A single number on the pH scale sits at the origin of this entire cascade.”
Your Skin Microbiome Has a pH Preference
The skin surface harbors a diverse microbial ecosystem. This community is not passive: it participates actively in barrier defense, immune calibration, and competitive exclusion of pathogens. Its composition is, to a significant degree, shaped by pH.
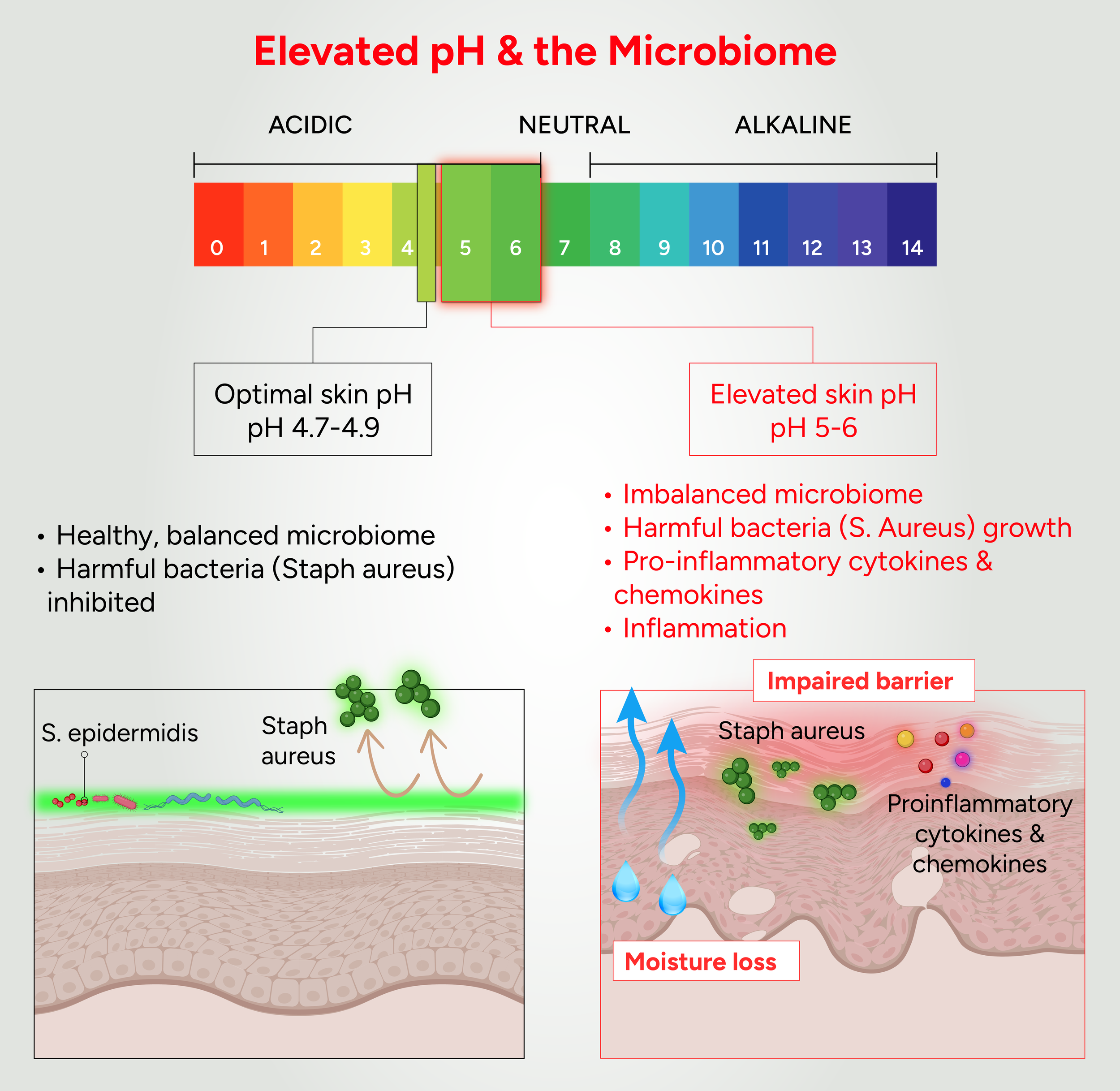
The dominant commensals on healthy skin — Staphylococcus epidermidis, Cutibacterium acnes, and related species — are adapted to thrive at the acidic pH of a healthy skin surface. Staphylococcus aureus, the pathogen most strongly associated with atopic dermatitis flares, grows preferentially at higher, more alkaline pH values. In vitro studies confirm the differential: conditions approximating the elevated pH of atopic skin favor S. aureus proliferation; acidic conditions favor the commensals (Iyer et al. 2021)
The acid mantle functions here as a selective filter. It creates conditions in which beneficial organisms flourish and pathogens are suppressed. But the relationship runs deeper than passive selection. Commensal bacteria metabolize the components of the acid mantle — sebaceous lipids, amino acids, natural moisturizing factor (NMF) constituents — and produce short-chain fatty acids, bacteriocins, and other metabolites that lower pH further, inhibit pathogen growth, and reinforce the barrier.
S. epidermidis, for example, produces proteases that selectively cleave biofilm- forming surface proteins of S. aureus, secretes lantibiotics that directly inhibit pathogen colonization, and generates fatty acids that acidify the local environment. In atopic dermatitis, where S. aureus dominates the skin surface during flares, this commensal defense network is largely dismantled (Liu et al. 2018).
“It is a positive feedback loop: host biochemistry supports the microbiome; the microbiome reinforces host biochemistry. When pH rises, both sides of that loop collapse at once.”
The Feedback Loop That Sustains Disease
Acid mantle disruption is a consistent feature across a wide spectrum of inflammatory and barrier-related skin disorders — atopic dermatitis, irritant contact dermatitis, Netherton syndrome, ichthyosis vulgaris, and aging skin, among others. Atopic dermatitis provides the most extensively studied example.
AD is a chronic inflammatory disorder characterized by pruritic, erythematous lesions and episodic flares. Its pathophysiology is multifactorial — encompassing barrier dysfunction, immune dysregulation, IgE-mediated hypersensitivity, and environmental triggers — but barrier impairment is considered the initiating event. Skin surface pH is elevated in AD, typically by 0.1 to 0.9 pH units, with reported values frequently ranging between 5.2 and 6.1. Importantly, pH elevation tracks disease severity in a predictable gradient: healthy skin < uninvolved skin in patients without active lesions < uninvolved skin in patients with active lesions < pre-lesional skin < lesional skin. This progressive alkalinization reflects both structural vulnerability and active inflammation.
The mechanism is self-reinforcing. Filaggrin deficiency — whether genetic or driven by inflammatory suppression of filaggrin expression — reduces endogenous acidifying capacity and weakens the buffering strength of the stratum corneum. The resulting pH elevation impairs lipid processing, enhances kallikrein activation, promotes microbial dysbiosis, and amplifies inflammatory signaling. Barrier breakdown facilitates microbial imbalance and cytokine release; inflammation further disrupts epidermal differentiation and acidification, sustaining elevated pH. The cycle feeds itself.
Interrupting this loop matters beyond the skin. Barrier dysfunction enables transcutaneous sensitization to allergens — a pathway implicated in the atopic march, wherein early-onset atopic dermatitis predisposes affected individuals to asthma, allergic rhinitis, or food allergies. Experimental models have demonstrated that maintaining an acidic stratum corneum prevents development of AD-like dermatitis in murine systems, and that topical acidification inhibits progression from dermatitis to aeroallergen-induced asthma. Alkalinization accelerates it. (Lee et al. 2014, Lee et al. 20215)
“pH elevation is not merely a consequence of inflammation. It is an upstream amplifier — one that activates proteases, dismantles the microbiome, and sustains the very inflammation it appears to follow.”
What Acidification Therapy Can and Cannot Do
If an alkaline skin surface drives so much pathology, the therapeutic question is obvious: can restoring acidity reverse it? The answer is yes — but the details matter considerably.
Hydroxy acids commonly used in topical formulations, such as glycolic acid and lactic acid, can transiently lower skin surface pH. However, their pKa values (approximately 3.8–3.9) lie well below the physiological skin pH range of ~4.5–5.0, limiting their ability to effectively buffer within the biologically relevant window. As a result, once the initial acidifying effect dissipates, skin pH tends to drift upward again.
Compounding this limitation, the small molecular size of these acids enables rapid penetration through the stratum corneum, which can provoke irritation in already compromised skin. At sufficiently low pH, hydroxy acids may also accelerate corneodesmosomal degradation and desquamation — mechanisms intentionally leveraged in chemical exfoliation, but potentially counterproductive in barrier-impaired conditions such as Atopic Dermatitis.
What compromised skin actually needs is sustained buffering capacity centered near pH 4.7 — a system that resists pH excursions over time rather than delivering a transient acid pulse. Effective formulations would ideally employ weak acids with pKa values aligned to the physiological set point, and with molecular structures large enough to remain at the skin surface rather than rapidly diffusing inward.
Beyond pH correction alone, an optimal strategy would also support the microbial ecosystem — incorporating prebiotic substrates that selectively favor commensal growth, and postbiotic metabolites such as short-chain fatty acids that contribute antimicrobial activity and reinforce the loop between microbiome ecology and barrier acidity.
“Acid mantle restoration can be safely combined with anti-inflammatory therapy, complementing immune suppression by addressing the underlying barrier and biochemical abnormalities that anti-inflammatory treatments do not directly correct.”
Most therapeutic strategies for Atopic Dermatitis have traditionally focused either on suppressing inflammation or providing passive barrier support through emollients and occlusives. While some topical formulations may transiently acidify the skin surface, there has historically been no practical technology capable of precisely restoring and sustaining the physiological acidic environment of the skin over extended periods. Soteri Skin was developed to address this gap through its pH/LOCK® technology, which is designed to restore and maintain the biochemical conditions of the acid mantle within the physiologically relevant range. In this way, it represents one of the first therapeutic approaches specifically engineered to directly target acid mantle dysfunction and chronic skin pH elevation as central components of disease pathophysiology.
This strategy is inherently complementary to immunomodulatory therapies such as dupilumab, JAK inhibitors, topical corticosteroids, and calcineurin inhibitors. While these treatments primarily target immune dysregulation and inflammation, they do not directly restore the biochemical environment of the skin surface, barrier architecture, or microbial ecology. In contrast, restoration of acid mantle integrity acts upstream and in parallel, helping normalize the acidic conditions required for optimal barrier function, enzymatic homeostasis, and microbiome balance. Used together, these approaches enable simultaneous targeting of multiple interconnected dimensions of disease — immune activation, barrier dysfunction, and microbial dysbiosis — potentially leading to more complete and durable disease control than either strategy alone.
A Final Note
The acid mantle has existed on the surface of human skin throughout human history, quietly and continuously maintaining the biochemical conditions required for healthy skin function. First described in 1928 as part of the skin’s antimicrobial defense system, it was long regarded primarily as a protective acidic coating. Only recently has it begun to be recognized for what it truly represents: a central regulatory interface governing barrier integrity, lipid-processing enzymes, protease activity, microbial ecology, and neuroimmune signaling — all simultaneously, all orchestrated through a remarkably thin acidic film maintained within a narrow physiological range.
It is not glamorous science. But it is foundational biology. The skin surface has a pH, and that pH profoundly influences everything that happens beneath it.