
We Tested the pH of the Most Popular Eczema Creams — Here's What We Found

The Question No One Is Asking
Walk through the skincare aisle and you’ll hear the same promises repeated: ceramides, colloidal oatmeal, shea butter, “barrier repair,” “dermatologist recommended.” This is the familiar language of eczema care—and of eczema marketing.
What you won’t see on the label is the one variable that may matter more than any of them: pH.
Healthy skin is not neutral—it is intentionally acidic. The surface of the skin operates optimally around pH ~4.7, and this acidity is not incidental; it is foundational. It governs a network of biochemical and structural processes that define barrier function, microbial balance, and sensory signaling. At this pH, the skin supports:
Ceramide synthesis through activation of key lipid-processing enzymes
Lamellar membrane organization, enabling an effective permeability barrier
Stratum corneum cohesion and integrity, preserving structural stability
Commensal microbiome balance, favoring beneficial over pathogenic species
Regulation of itch signaling, including suppression of pH-activated proteases
In atopic dermatitis, this system is disrupted at its foundation. Skin surface pH is consistently elevated—often reaching 5.2 to 6.0 or higher on lesional skin. This shift may seem small numerically, but biologically it is profound, altering enzyme activity, weakening barrier structure, and amplifying inflammatory and itch pathways.
Which raises an uncomfortable but critical question:
What happens when you apply a moisturizer with a pH of 5.5, 6.0, or even 6.7 onto skin that is already pathologically elevated in pH?
To explore this, we measured the pH of some of the most widely used eczema creams on the market.
What We Tested — and What We Found
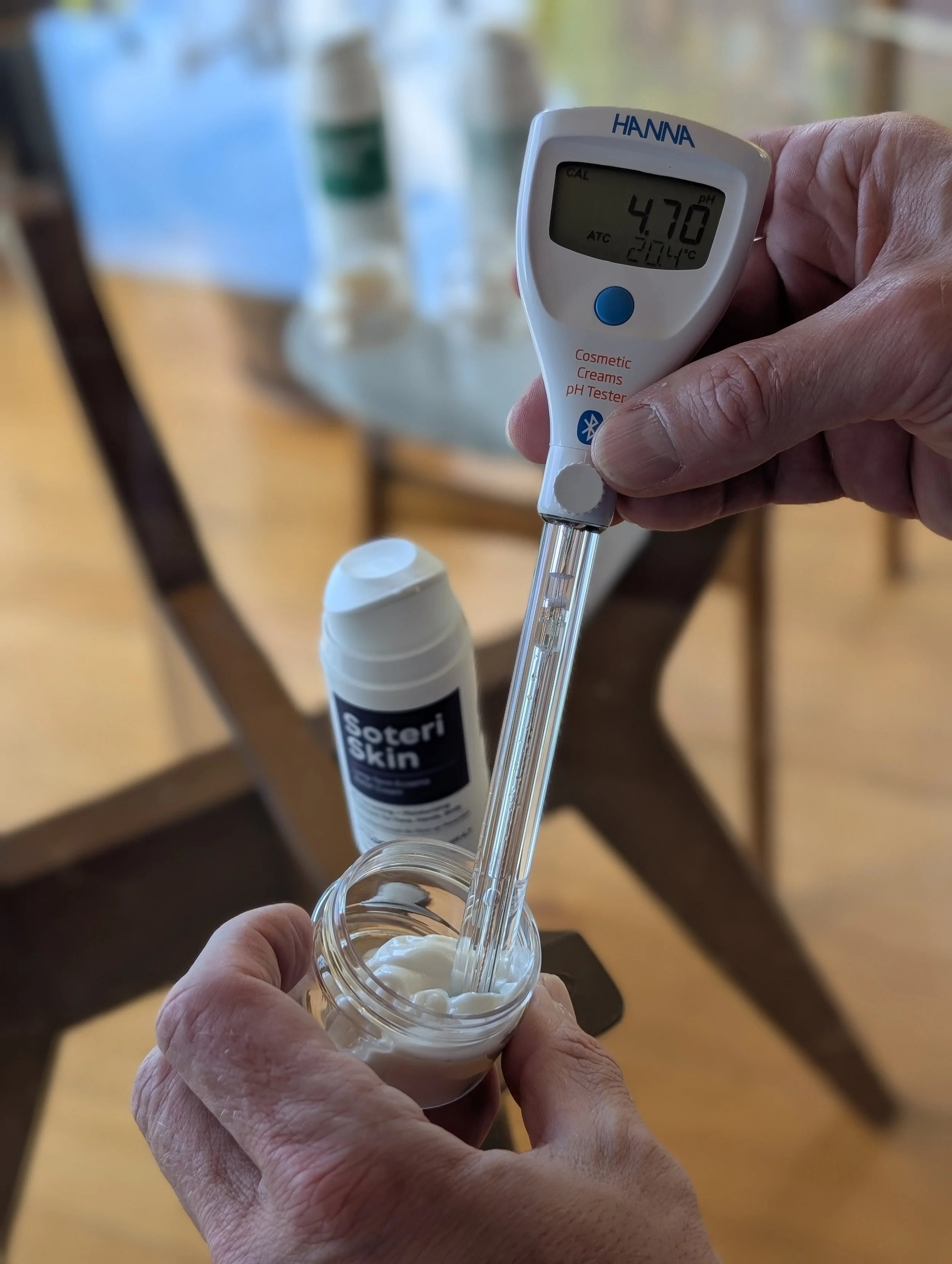
Using calibrated pH instrumentation under standardized conditions, we measured the following products:
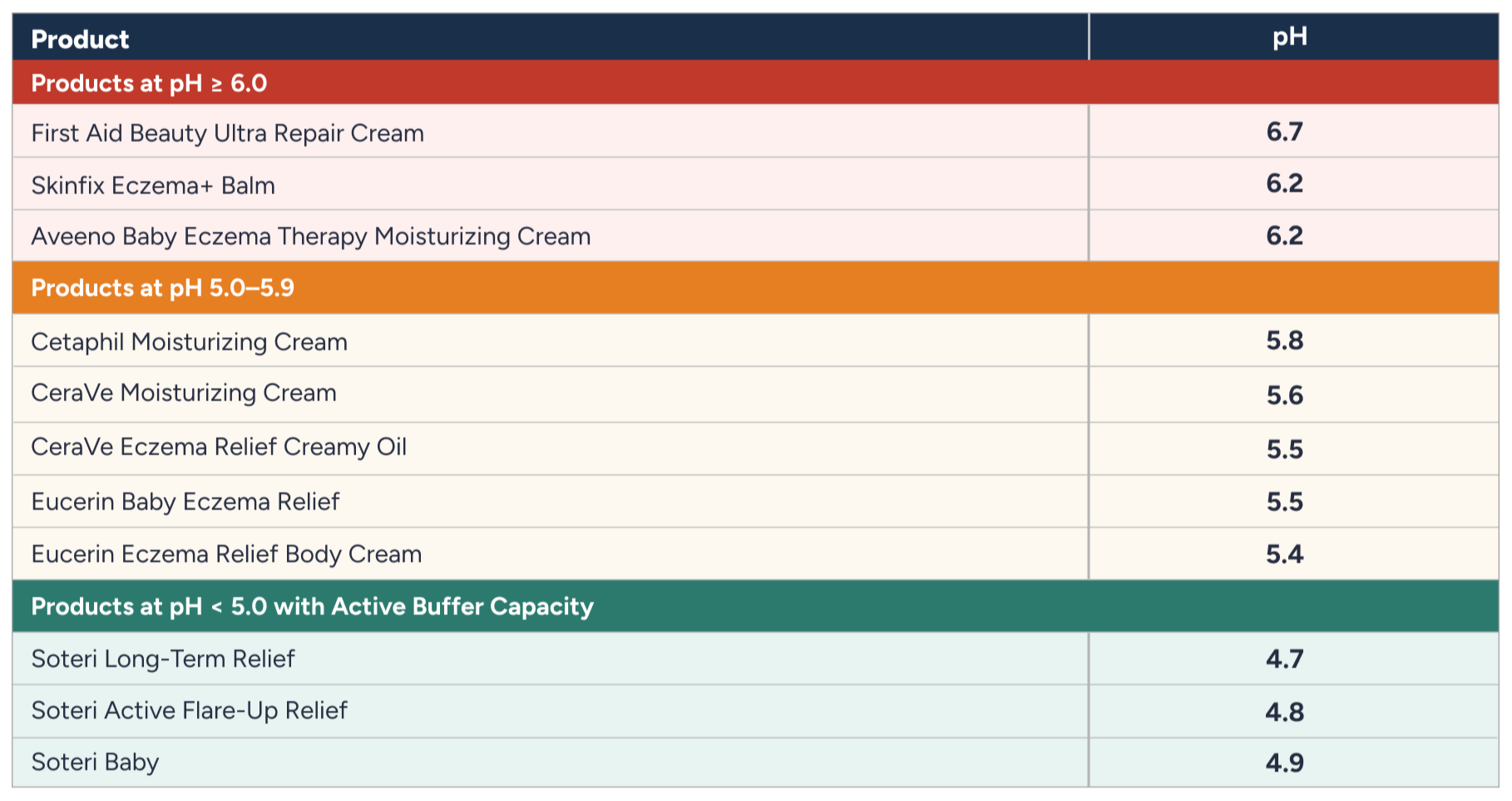
“The pattern is striking. The overwhelming majority of popular eczema creams sit above the physiological pH range of healthy skin. Many sit significantly above it.”
Why pH Is Not Just Another Formulation Detail
A difference of 0.5 or 1.0 pH units sounds trivial. It is not — because pH is logarithmic. Each unit represents a tenfold change in acidity. Small numerical shifts produce large biochemical consequences.
There are three mechanisms through which this plays out in eczematous skin.
1. Lipid-Processing Enzymes
Two enzymes are responsible for ceramide production within the stratum corneum: β-glucocerebrosidase and acidic sphingomyelinase. Both have acid-optimized activity profiles. As surface pH rises above 5.5, their efficiency declines, ceramide conversion becomes incomplete, lamellar membrane architecture becomes disorganized, and barrier recovery slows.
“Atopic skin is already ceramide-deficient. A moisturizer applied at pH 5.5–6.7 does not create conditions for enzymatic correction — it applies ceramides into a biochemical environment that cannot process them optimally.”
2.Serine Proteases and the Itch Signal
Kallikrein-5 (KLK5) and kallikrein-7 (KLK7) govern normal skin cell turnover. Under acidic conditions, their activity is restrained. As pH rises, KLK activity increases exponentially — corneodesmosomes degrade prematurely, stratum corneum cohesion weakens, and microfissures develop.
More critically, KLK5 activates protease-activated receptor-2 (PAR2). PAR2 activation triggers TSLP release, pro-inflammatory cytokine cascades, and direct sensory nerve stimulation. This means elevated pH doesn't just impair barrier function — it actively amplifies the itch signal, independent of visible inflammation.
“This is the protease–pH–itch axis: a self-reinforcing loop in which elevated pH feeds forward into itch, which feeds forward into scratching, which feeds forward into barrier damage and further pH elevation. Moisturizers are supposed to interrupt this loop. Applied at pH 5.5 or above, they may not.”
3.Microbial Ecology
Skin acidity is a key determinant of microbial balance. At pH 4.7–4.9, commensal organisms thrive, colonization resistance is maintained, and organic acid production from commensals reinforces the acidic environment. Above pH 5.5, Staphylococcus aureus persistence increases, its virulence factors become more active, and dysbiotic shifts become more likely.
Multiple published studies have documented the correlation between elevated skin pH and S. aureus colonization in atopic dermatitis. A cream applied at pH 6.2 or 6.7 does not challenge this dynamic — it accommodates it.
The Specific Problem With pH ≥ 6



Three products in our testing registered at or above pH 6.0: Aveeno Baby (6.2), Skinfix (6.2), and First Aid Beauty (6.7).
To appreciate what that means in practice: at pH 6.7, a product is more than 100 times more alkaline than the physiological target of 4.7.
Applied to eczema-prone skin where protease activity is already elevated, barrier recovery is already impaired, and microbial imbalance is already present, a product in the 6+ range sustains kallikrein activation, delays ceramide regeneration, and creates a permissive environment for dysbiosis.
This is not a judgment about the intentions behind these formulations. Colloidal oatmeal, ceramides, and anti-inflammatory ingredients are not inert — they may confer real benefit. But ingredient lists do not override biochemical environments. The vehicle pH determines whether those ingredients can function as intended.
The More Complicated Case: pH 5.4–5.8


The cluster of products at pH 5.4–5.8 — Eucerin, CeraVe, Cetaphil — represents the industry's current center of gravity. These are better. They are not optimal.
At pH 5.5, β-glucocerebrosidase activity is measurably reduced relative to pH 4.8. KLK activity is higher than at physiological acidity. Re-acidification of already-elevated atopic skin may be incomplete. For non-eczema skin, pH 5.5 is likely tolerable. For atopic skin already shifted upward, maintaining the surface at 5.6–5.8 may not restore the enzymatic and microbial balance that healthier skin achieves at 4.7.
“This doesn’t mean these products cause harm. It means they may not address the upstream biochemical problem.”
Measured pH vs. Active Buffer Capacity
There is an important distinction that pH measurements alone don't capture.
A product that reads pH 4.8 in the bottle is not necessarily a product that maintains skin pH at 4.8 after application. Skin has buffering capacity. Eccrine secretions, sebum, metabolic byproducts, and ambient moisture all interact with applied products. A formulation without intrinsic acid-buffering capacity will be neutralized over time.
Active buffer capacity describes a formulation's ability to resist pH drift — to maintain acidic conditions on the skin surface even in the presence of competing buffering forces. This is distinct from pH at time of application.



The Soteri products tested here — Long-Term Relief (4.7), Active Flare-Up Relief (4.8), and Baby (4.9) — sit within the physiological equilibrium range of healthy skin. They are also design to maintain pH in this optimal range over several hours. The goal in atopic skin is not a transient acidification event but sustained stabilization within the 4.7–4.9 range.
Why This Matters More in Infants
Infant skin is not a smaller version of adult skin. The stratum corneum is thinner, barrier function is less mature, buffering capacity is reduced, and transepidermal water loss is inherently higher. Products marketed for baby eczema — marketed specifically for a more vulnerable barrier — at pH 6.2 may not support acid mantle restoration in the patients who need it most.
Early-life barrier instability has been linked to higher risk of atopic disease progression. If acidic surface pH is a precondition for normal barrier function, maintaining it during infancy is not a refinement — it is a mechanistic priority.
Summary
The data from this testing can be organized simply:
“Most widely used eczema creams cluster into two distinct pH ranges. The majority fall between pH 5.4–5.8—already meaningfully above the skin’s physiological acidity—while a substantial number reach pH 6.0 and higher, placing them clearly outside the optimal range for atopic skin.”
For eczema-prone skin, where surface pH is already elevated relative to healthy baseline, this difference is not cosmetic — it is mechanistically relevant to enzyme activity, protease regulation, itch signaling, and microbial ecology.
The Takeaway
Eczema management tends to focus on what goes into a product — steroids, biologics, ceramides, anti-inflammatory actives. But ingredient function is not independent of the biochemical environment in which those ingredients are applied.
Surface pH determines whether ceramide-synthesizing enzymes can operate. It determines whether serine protease activity is suppressed or amplified. It determines whether the microbial environment shifts toward commensals or toward S. aureus. These are not marginal effects. They are the foundational conditions for barrier function.
Products with pH at or above 6.0 may be particularly suboptimal for atopic skin, operating in a range associated with protease activation, microbial imbalance, and impaired barrier recovery. Products in the 5.4–5.8 range are better but still above the physiological target.
For patients managing eczema — especially moderate-to-severe atopic dermatitis, and especially in children — pH should be considered a primary formulation parameter. Not an afterthought. Not fine print.
“Not all moisturizers are biochemically equal. The pH tells you a great deal about why.”
© Soteri Skin | soteri.com | Science-backed eczema relief